A 65 yr old male with abdominal pain
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome .
understand the topic of “ patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Patient came to OPD with chief complaints of pain abdomen since 4 days
HOPI :
Patient was apparently asymptomatic 4 days back then he developed pain in the abdomen, insidious in onset, gradually progressive dragging type,aggravated on doing work ,after sudden increament in the consumption of alcohol (90ml to 180ml)not associated with nausea,vomitings
No h/o constipation
H/o burning micturition
Past history
N/k/c/o HTN, Asthma, epilepsy,TB , CAD,CVA
No h/o surgeries in the past
No H/O blood transfusion
No h/o radiation exposure
Personal history: patient is farmer by occupation
Diet mixed
Appetite decreased since 4 days
Sleep adequate
Bowel and bladder regular
Burning micturition
Addictions regularly consumes alcohol about 90 ml/2day Since 30 years
Daily routine:-
Patient wakes up at 6:00am approx. and goes for walk for 1hour and freshen ups and have a cup of tea and goes for farming then he will have his lunch at 2:00 and then comes back home around 5:00 and have tea and have dinner at around 8:00 and goes to bed at 9:00
Alcohol comsumption every alternate days
General physical examination
Pt is conscious coherent cooperative well oriented to time place person
Moderately built and nourished
Vitals
BP : 130/80 mm Hg
PR : 69 bpm
Spo2 98 on RA
Temp: 98.3 F
GRBS 197 mg/dl
No pallor, cyanosis, clubbing,
lymphadenopathy,edema
Icterus present
Systemic examination :
Cvs- s1 ,s2 heard
CNS- no focal neurological deficits noted
Rs -BAE + , NVBS
P/A
Inspection : abdomen flat
No scars,sinuses,hernial orifices, pulses,masses,
All quadrants are moving equally with respiration
On palpation:
All inspectory findings are confirmed
Abdomen soft
Tenderness in epigastric and both hypochondriac regions
No local rise of temperature
On percussion:
No fluid thrills no shifting dullness
Tympanic note heard
On auscultation :
Bowel sounds heard
Investigation:-
CBP:-

Serum lipase:-

LFT

AMYLASE

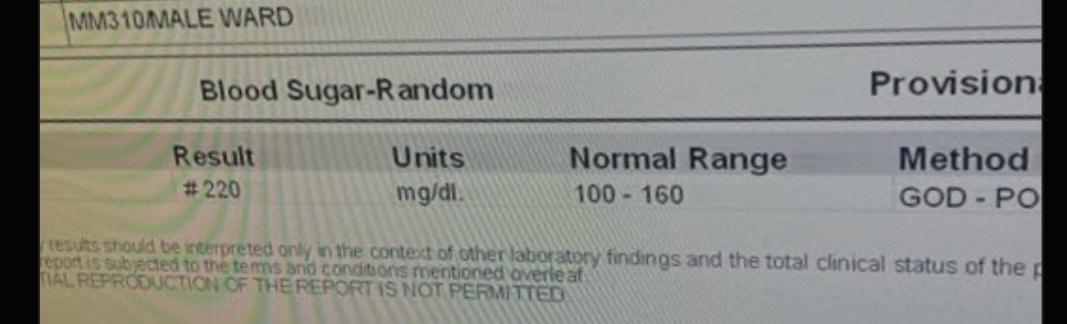
RBS
USG abdomen and pelvis

Chest X ray

X ray abdomen

Provisional diagnosis : acute on chronic pancreatitis
Treatment:-
Inj ceftriaxone 2 g /IV / BD
INJ METROGYL 500 mg IV /TID
Inj thiamine 200 mg in 100 ML NS IV/tid
Inj Tramadol 100 mg in 100 ML NS IV/BD
INJ PAN 40 Mg IV /OD
INJ ZOFER 4 Mg IV /BD

Comments
Post a Comment